


Introduction
Essential tremor (ET) is a progressive neurological disorder that affects about 0.9% of adults, with a known increasing of prevalence with age [1].
ET is characterized by postural and/or kinetic tremor, affecting the upper limbs, head and possibly voice; there is evidence that other neurological disturbances (‘non-motor’ symptoms) such as mild cognitive changes, depression and olfactory and hearing deficiencies occur more frequently in patients with ET compared with age-matched controls [1]. Pharmacological treatment consists of propranolol, primidone and topiramate, which obtains a 50% reduction in tremor severity in 70% of patients; benzodiazepines, topiramate and gabapentin have been suggested as second-line therapy [1]. Surgical ablation targeting the ventral intermedius nucleus of the thalamus (VIM) was among the first stereotactic procedures and proved highly effective for treating medication-resistant tremor, recent approval of magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy for the treatment of ET has ignited the debate surrounding the use of incisionless thalamotomy [2,3]. Voice, central head tremor patients shows bilateral thalamic deep brain stimulation (DBS) [2,3].
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement [4]. A search of PubMed, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials and Scopus databases was conducted to identify articles of interest. These databases were searched using the following terms: “essential tremor”, “essential tremors and ventral intermedius nucleus”, “essential tremor and deep brain stimulation”, “essential tremor and high intensity focused ultrasound”, “essential tremor and GammaKnife”. Giordano et al. [5] also considered tremor severity at presentation and at follow-up visits, impact of tremor on quality of life (QoL) and/or activities of daily living at presentation and at follow-up visits. When a study reported outcomes at more timepoints, the outcome at 12 months (or, in its absence, the closest timepoint available) was considered.
Each study employed validated scales in the preoperative and postoperative settings to gauge the changes in tremor severity and/or QoL as an expression of treatment efficacy. The heterogeneity of rating scales did not allow for a direct comparison between the DBS group and the MRgFUS group. Therefore, improvement was defined by the percentage change between preoperative and postoperative scores [6]. Indications for the use of MRgFUS as a treatment option for patients with ET include of following criteria: confirmed diagnosis of essential tremor, failure to respond to, intolerance of, or medical contraindication to use of at least 2 medications for ET, 1 of which must be a first-line medication, appendicular tremor that interferes with QoL based on clinical history, unilateral treatment, contraindication to use of MRgFUS: bilateral MRgFUS thalamotomy, contralateral to a previous thalamotomy, cannot undergo magnetic resonance imaging (MRI) because of medical reasons, skull density ratio (ratio of cortical to cancellous bone) is <0.40 (Table 1) [7].
There are several case series of GammaKnife thalamotomies in the literature for patients with ET. The largest series of GammaKnife thalamotomy for ET presented the results of 161 patients, who underwent a total 203 thalamotomies (119 unilateral and 42 bilateral). The vast majority of patients were treated with 140 Gy, varying from 140 to 150 Gy, using a single isocenter and 4 mm collimation. Overeall, 81% of patients showed improvements in drawing and 77% showed improvement in writing scores. There were 14 patients who suffered neurologic side effects that were temporary (6 patients) or permanent (8 patients), which accounted for 6.9% of the 203 treatments (Table 2) [8-13]. Okun et al. [13] reported a higher rate of complications in series of 8 patients; 7 of whom were treated with maximum doses of 200 Gy. Most neurosurgeons perform radiosurgical lesioning for functional disorders at lower doses (e.g., 140 Gy).
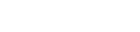
Plugging pattern is used avoiding for high doses to shot to internal capsule (Fig. 1). There were 517 complications reported in the DBS group and 484 complications reported in the MRgFUS group. The MRgFUS group had a higher prevalence of gait disturbances/muscle problems, paresthesias and nausea, while the DBS group had a higher prevalence of speech disturbances and local adverse symptoms [14]. No deaths were reported in the MRgFUS group, while one surgery-related death was reported in the DBS group: the patient developed a small intracerebral haematoma soon after implantation of the test electrode. This caused decreased consciousness and was followed by aspiration pneumonia and, ultimately, by respiratory failure. Lead-related complications and speech disturbances were the most common adverse event observed in the DBS group [14]. In the MRgFUS group, only 26 cases of postoperative speech disturbance were registered (5.5% of all adverse events); adverse events of sensory nature were the most common, closely followed by gait disturbances/muscle problems [14]. Twenty-six studies stated whether the reported complications were transient or persistent (present at the latest follow-up), including 288 patients treated with MRgFUS and 678 patients treated with DBS [14]. Complications were more frequently persistent in the MRgFUS cohort than in the DBS cohort (Table 3) [14].
In our study, GammaKnife radiosurgical nucleus ventralis intermedius thalamotomy using the gamma knife unit was performed to make lesion in 7 ET patients. Male to female ratio was 5:2. A mean radiation dose of 100 (80-120 Gy) was delivered to nucleus using a single 4-mm collimator plug pattern following classic anatomical landmarks. Mean age was 72 (65-77) years. Patients were followed for a median of 31.5 months (range, 7-60 months). Ventralis intermedius thalamotomy produced an excellent improvement of the tremor in 6 cases, one 69-year-male patient initially improved, but 10 months later, tremor was recurred and he received re-GammaKnife thalamotomy. It showed improved tremor symptom in geriatric age of the essential tremor patients. There was no complication after gamma knife surgery.
Treatment Modalities
Essential tremor is one of the most common movement disorders. The prevalence of this progressive neurological disorder increases with age: in the general population, the prevalence is 0.9%, rising to 4%, in adults aged 65 or older [15,16]. ET is characterized by a distinctive postural and intention tremor typically affecting the hands more than the legs, trunk, head or voice [2,17]. ET does not shorten life expectancy, but it can affect QoL, functional activities, mood and socialization [18].
High level of evidence exists for propranolol and primidone as first-line medications that reduce tremor by approximately 60% in 50% of patients [19]. Daily doses of 30 to 240 mg of propranolol, <30 to 500 mg of primidone, 400 to 800 mg of topiramate are recommended [19]. Other drugs include gabapentin, carbonic anhydrase inhibitors, clozapine, flunarizine, clonidine and the methylxanthine-derivative theophylline [20]. However, up to 30% of patients do not respond to first-line therapy or may experience intolerable adverse effects [19].
Radiofrequency lesioning is a functional neurosurgical technique performed with a special electrode through which high frequency current produces a local heating of the tissue at the tip of the electrode above 60 degrees leading to the destruction of all cells and fiber tracts in the target region. The improvement of the lateralized outcomes is 84% and for the tremor total score around 74% with very few data [21-24]. The most important limitation is the irreversibility of the procedure and the higher adverse event rate.
Neurosurgical thalamotomy used to be the treatment of choice for patients with drug-resistant incapacitating tremor, with an effectiveness between 73% and 93% [23]; however, the permanent complication rate ranged between 9% and 23% [23]. DBS is a functional neurosurgical technique by which a permanent electrode with 4 to 8 contacts is implanted to the Vim of the thalamus with stereotactic planning of the target with or without confirming the target area with microelectrodes in the awake patient [17,25]. The stimulator is implanted subcutaneously in the subclavicular area and a subcutaneously implanted wire connects to the electrode. The current applied through the contacts of the permanent electrode is blocking cells and fibers in the target area and the radius of this functional and reversible blockade is depending on the strength and pulse characteristics. It is currently the standard of surgical interventions for tremor axial tremors (head and voice tremor) are known to be less responsive to medical but also surgical treatments [19] than extremity tremors. Particularly, unilateral DBS was found less efficient than bilateral DBS in several studies for head and voice tremor [19] which has led to the recommendation of bilateral procedures in case of axial tremors. Radiosurgery is done in the radiation suite and uses focal radiation to destroy the tissue in the target area, again in the well-defined Vim through imaging of the rigidly fixed head.
During GammaKnife thalamotomy, patients are placed in a stereotactic frame under local anaesthetic. Typically, a single central maximal dose of 130 to 152 Gy using a 4 mm collimator is administered to the Vim. Optimal planning minimises radiation exposure to the internal capsule [21,24,26].
Several authors suggest that staged bilateral stereotactic (SRS) radiosurgery can be performed safely, although the documented experience is limited to only 51 patients with ET. Long-term effects of 17 out of 52 patients which were followed up to 4 years were reported to be stable [2]. Side effects are reported to be as rare as 0.7% in a recent meta-analysis. At least they are highly variable and cases with running lesions and further complications do not show up in the reports. They are reported for single cases [13,27]. Radiosurgery is carried out unilaterally in the majority of cases. The surgery is inexpensive compared to other methods.
A major drawback of radiosurgery or essential tremor is the lack of intraoperative clinical or electrophysiological aids to account for differences between individuals [28]. Tractography can be of benefit to localize the Vim and internal capsule during target planning [3,14,29]. The delayed therapeutic effect is another important issue; benefits may not be present up to 1 year after SRS, with a median time of approximately 4 months [30,31].
MRgFUS is using 1,024 synchronized ultrasound emitters which are focused to a single point. When the temperature increases above 50°C, the protein is denatured and the cells and fibers are irreversibly destroyed [17,25].
The head, again rigidly fixed in a stereotactic frame, is placed exactly with the target area into this focus. Identifying the target area is done analogously as with the above mentioned techniques. The patient is brought into the MRI where the procedure takes place under image guidance. The Vim nucleus is targeted stereotactically, and US energy is delivered in progressive doses until focal target temperatures are achieved, causing permanent cell death. The procedure is monitored with magnetic resonance thermometry, and the patient is awake for intraprocedural tremor assessments [32].
Confirmation of the target with microelectrodes is not possible due to the incisionless technique, but this can be replaced by heating the target region to 48°C which reversibly inactivates the tissue and thereby the effect on tremor can be tested clinically before a definite lesion is placed with higher temperature. The head has to be carefully shaved for this procedure [32].
Giordano et al. [5] found MRgFUS to be inferior to DBS in terms of tremor severity improvement. Perioperatively, stereotactic procedures may result in intracranial haemorrhage, which is arguably the most severe complication that may ensue. This risk primarily arises from the introduction of the electrode and the potential disruption of vessels along the trajectory.
The most commonly encountered adverse effects were Paresthesias involving the face, lips or fingers (27% of patients in total, 19% transient, 8% persistent beyond 1 month) [33]. This is secondary to inadvertent heating of the adjacent somatosensory thalamus. The second most common complication was ataxia and gait instability (23% overall, 19% transient, 4% persistent) [33,34]. Many patients with ET have mild gait disturbances preoperatively, which are temporarily worsened after thalamotomy. More uncommonly, transient (2%) and persistent (2%) hand or face weakness was apparent due to heating of the internal capsule. Other less common complications were transient ischaemic attack, hypogeusia, persistent finger dysaesthesia and deep venous thrombosis requiring anticoagulation (1% each). Among current reports, 8 patients (7.5%) experienced treatment failure secondary to insufficient heating at the target to create an ablation [35,36].
Elderly patients have been thought to recover at a slower rate from surgery and to be at a higher risk of developing postoperative neurologic complications [37-39]. Over 70 years old, now we called old age, in old age intractable essential tremor, minimal invasive GammaKnife thalamotomy or MRgFUS thalamotomy is needed and increasing state.
Conclusion
Since DBS has been safely used for decades, it is considered by many surgeons and neurologists to be the treatment of choice for most patients with medically refractory or severe ET in pre-geriatric age.
Gamma knife surgery thalamotomy has been performed for several decades by several groups, but has received some criticism since there are no means for intraprocedural target confirmation and delayed treatment effects. GammaKnife thalamotomy is effective for geriatric intractable ET patient. FUS thalamotomy is the newest modality for tremor treatment and has received attention since it has transcranial capabilities, immediate effects and the potential for procedural target refinement.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






