Cage dislodgement as a severe complication after anterior cervical discectomy and fusion: a case report
Article information

Abstract
Anterior cervical discectomy and fusion (ACDF) is a common treatment for patients with diverse cervical spine pathologies. Despite its favorable outcomes, numerous complications are still existing. In this case report, we present a complication involving cage dislodgement following ACDF in a patient with cervical trauma. A 62-year-old man presented at our hospital with right arm weakness following a fall injury. Radiographic evaluation revealed a fracture of the right C5 lamina, a fracture of the C6 transverse process, and a ruptured disc with downward migration, leading to spinal cord compression and right foraminal stenosis. The patient underwent ACDF at the C5–6 level, resulting in improved symptoms and subsequent discharge. However, 2 months after, dislodgement of the cage occurred, leading to C5–6 spondylolisthesis. Nonetheless, no further deterioration of neurological function was observed. Without additional surgery, the patient's condition was monitored over the course of 1 year, during which time bone fusion was deemed to have successfully taken place. Routine X-rays are crucial for the regular monitoring of post-surgical ACDF patients, especially those with traumatic cervical injuries. If cage dislodgement and spondylolisthesis develop without worsening symptoms and with minimal impact on the spinal canal, close observation may be favored.
Introduction
Anterior cervical discectomy and fusion (ACDF) is recognized as one of the most frequently conducted spinal procedures. The clinical outcomes of this intervention are predominantly favorable, with the majority of cases demonstrating good or excellent results [1–6].
In spite of its well-established effectiveness, this procedure carries the possibility of complications. Esophageal perforation, vertebral artery injury, dural tears, spinal cord injury, recurrent laryngeal nerve injury, and dysphagia are recognized complications associated with this approach.
Additional concerns that could arise during the postoperative period encompass pseudarthrosis, adjacent segment disease, as well as implant subsidence or extrusion [7–9]. These complications have the potential to lead to considerable patient morbidity and frequently necessitate revision surgery to ensure appropriate management.
In this report, we present a case of a patient who underwent C5–6 ACDF following severe cervical trauma. This case is noteworthy for a rare complication involving the vertical dislodgment of the interbody cage. Interestingly, despite the absence of additional surgery, follow-up X-ray imaging revealed successful bony fusion at the C5–6 level, and no deterioration of symptoms was observed.
Case Report
A 62-year-old man, who had a history of rectal cancer operation, 3 m fell down backward during working on the ladder. He presented with right hemiparesis (Motor grade 3), particularly right forearm and finger (Motor grade 1) (American Spinal Injury Association scale D) and right arm paresthesia.
Imaging studies were obtained, including simple spine X-rays and a computed tomography scan, which revealed a severe traumatic injury to the cervical spine. There was a fracture of the right C5 lamina and bilateral lateral mass fractures, with no evidence of facet dislocation observed (Fig. 1). Magnetic resonance imaging revealed evidence of a ruptured disc at the C5–6 level, with a fragment showing inferior migration. This condition led to spinal cord compression, as well as central and bilateral foraminal stenosis (Fig. 2).
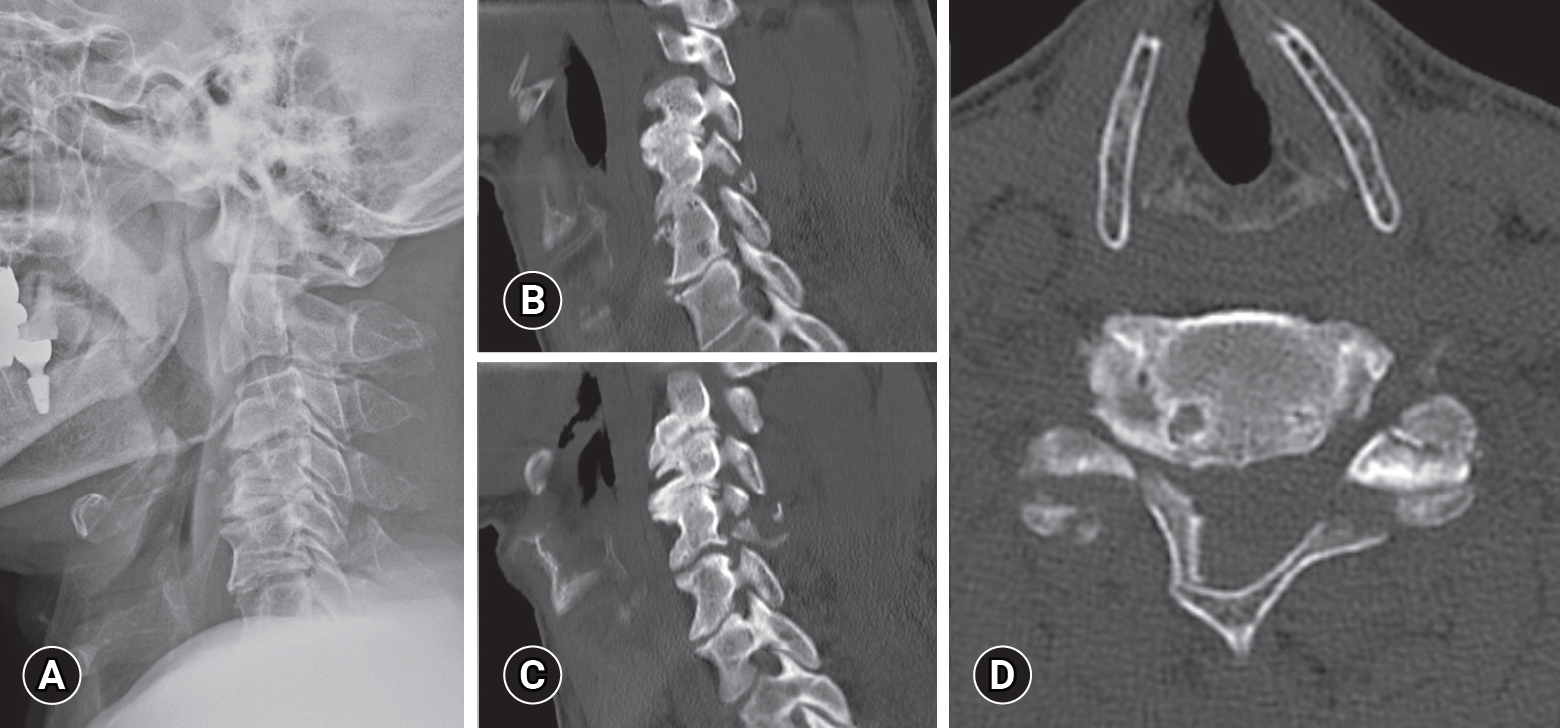
Initial simple spine X-ray (A) and sagittal right (B), left (C), and axial (D) computed tomography scans show a bilateral lateral mass and lamina fracture.
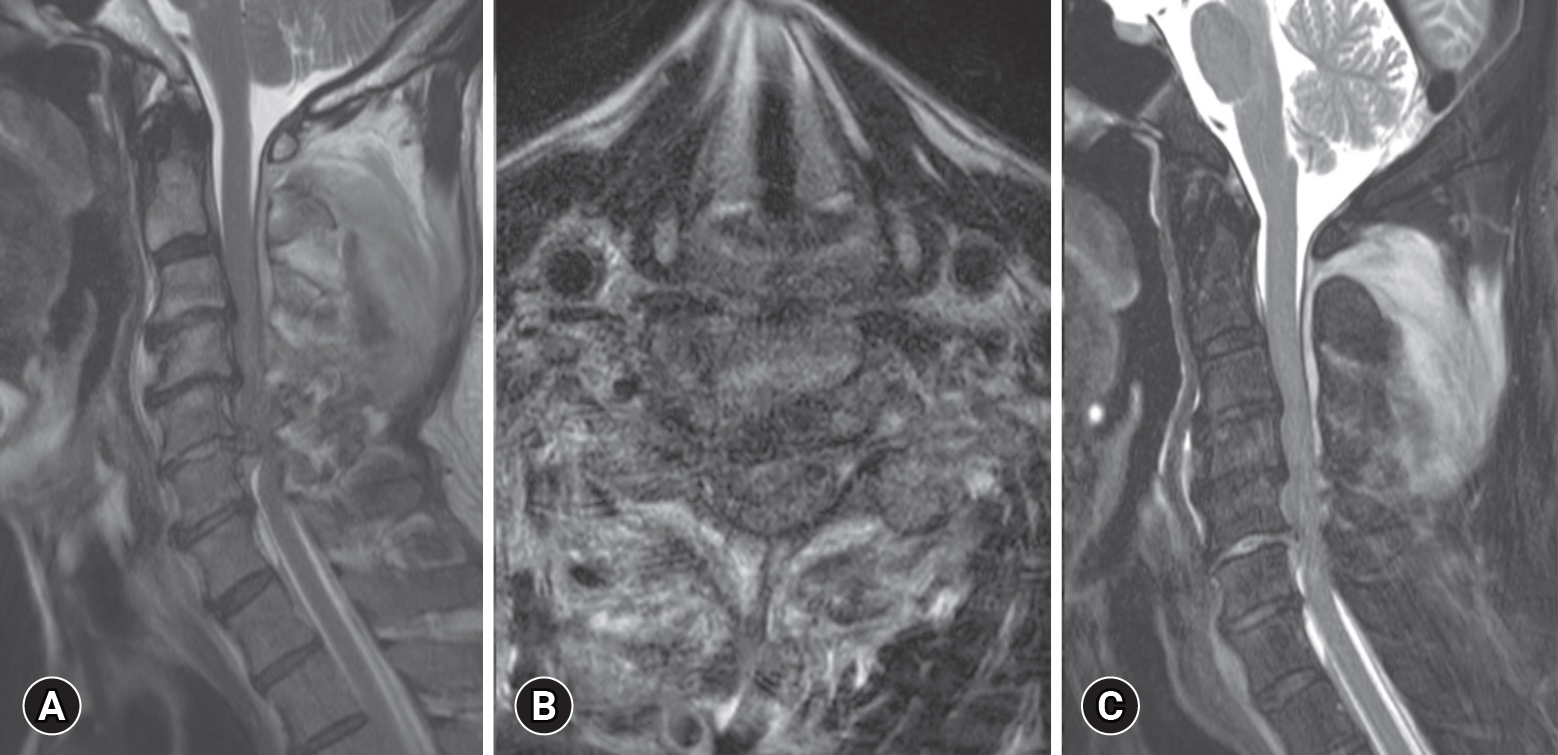
Initial T2 sagittal (A), axial (B), and fat suppression (C) images show C5–6 severe cord compression due to ruptured disc, anterior epidural hemorrhage, C5–6 bilateral foraminal stenosis, and severe posterior ligament complex injury.
Given the significance of his symptoms and imaging, along with physical exam findings consistent with spinal cord injury, surgical intervention was selected. Emergency surgery of C5–6 ACDF with an allogeneic bone interbody cage and plate fixation was decided upon due to the patient's paralysis, and the procedure commenced five hours after their arrival in the emergency room. The procedure was carried out through an anterior Smith-Robinson approach localized over the C5–6 disc space. Once the correct level was identified, a complete discectomy was conducted, followed by central and foraminal decompression with the removal of the disc fragment. Appropriately sized integrated plate/cage devices were then placed. The device had been pre-filled with Demineralized bone matrix. 4 screws, bilaterally cranial and caudal, were predrilled and placed into the plate. Fluoroscopy confirmed that the cages, plate and screws were in proper position and the wound was irrigated and closed in layered fashion.
Postoperatively, there was no evidence of any immediate complications. The patient was fitted with a rigid cervical collar (Philadelphia cervical brace) and it was planned to be worn for a minimum of 3 months.
The patient was discharged one month after the surgery. Rehabilitation was concurrently initiated during the hospitalization period, resulting in an improvement in the patient's muscle strength (from grade 3 to 4) and enabling ambulation. Nonetheless, the right arm paresthesia persisted. The dislodgment of the cage occurred during a follow-up outpatient visit at the 2-month after surgery. The cervical anteroposterior and lateral X-ray images revealed the dislodgement of the cage, characterized by vertical rotation and posterior migration into the spinal canal. Additionally, there was evidence of C5–6 spondylolisthesis, accompanied by failure of the C6 plate screws. Despite the occurrence of cage dislodgement and spondylolisthesis, the space within the spinal canal remained relatively unaffected, and there was no exacerbation of symptoms (Fig. 3). considering the risk of spondylolisthesis worsening, we suggested further posterior surgery, but the patient declined. Consequently, no additional surgery was performed, and after a year of follow-up, bone fusion is presumed. The patient had provided permission to publish these features of his case, and the identity of the patient has been protected.
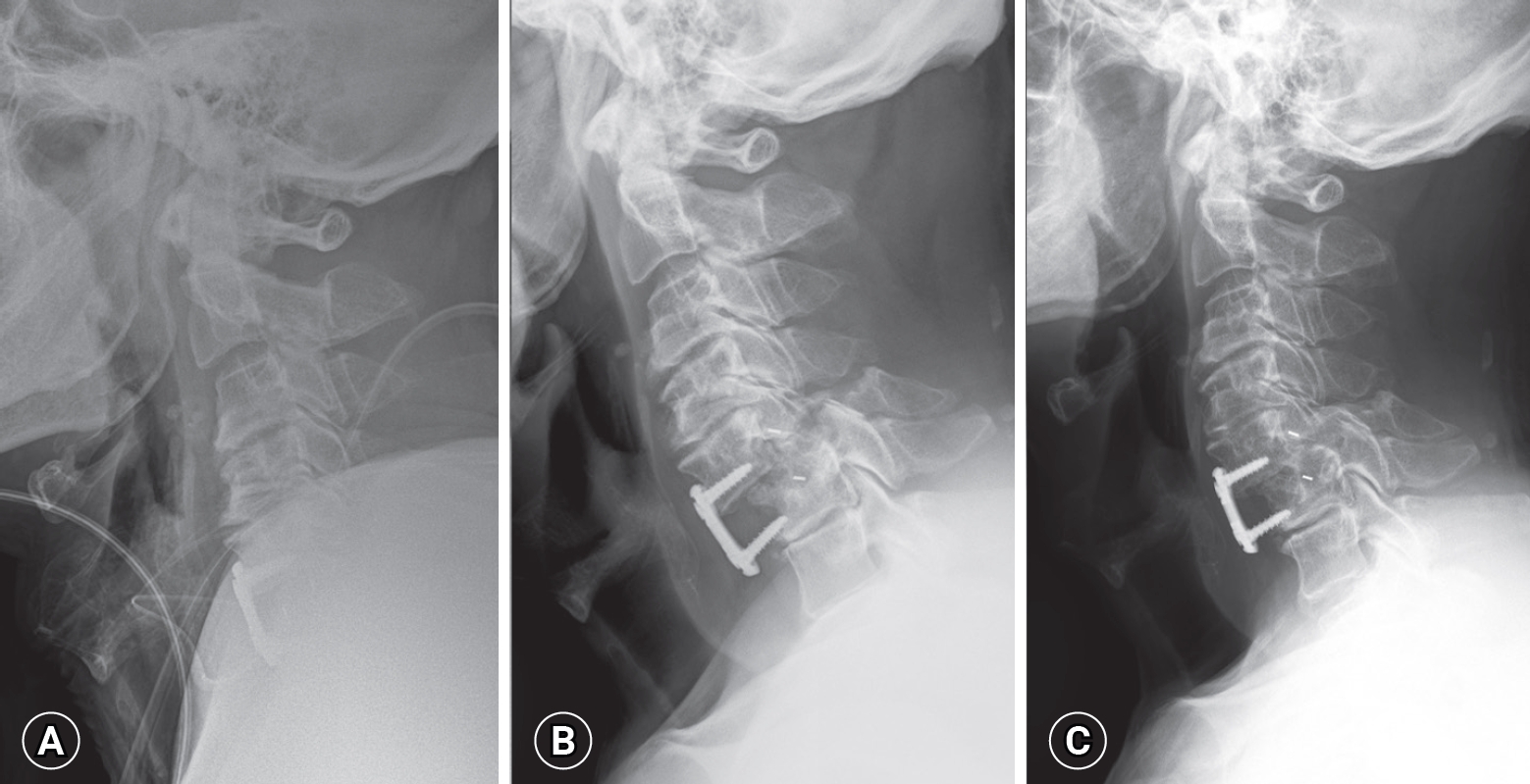
Serial simple spine X-ray images show (A) the immediate postoperative state, (B) the occurrence of cage dislodgement and spondylolisthesis 2 months after surgery, and (C) a stable fusion state 1 year after surgery.
Discussion
Surgical treatment for cervical facet dislocations varies widely and includes options such as anterior, posterior, anterior-posterior, posterior-anterior, and anterior-posterior-anterior approaches [10,11]. Among these approaches, the anterior-only approach, which involves closed or open reduction, discectomy, and instrumental fusion, is particularly recommended. This is especially true when a traumatic intervertebral disc herniation is present and there is no spinal cord injury [12–16]. However, achieving satisfactory reduction can be challenging in cases involving bilateral locked facets. Data from biomechanical and clinical studies have reported that anterior fixation has less stability than posterior fixation [17,18] and that there is also hardware failure of unicortical anterior plating [19].
Nevertheless, in our specific case, bilateral facet injury was present without clear dislocation or instability. This led us to consider that ample stability could be achieved through an anterior-only surgical approach, combined with the use of a neck collar to ensure maintenance. However, it is noteworthy that numerous recent studies have raised questions regarding the necessity of cervical collar usage. Cervical bracing, also referred to as cervical orthosis or a hard collar immobilization, is a frequently employed component of spinal care following trauma [20]. Additionally, it may serve as a supplementary measure during the recovery period following elective cervical spine surgery.
Anecdotal reports suggest that elective use is justified with the expectation that bracing reduces the risk of non-union and pain, providing patients with a subjective sense of security. While these assumptions are widely held, a growing body of evidence indicates that hard collar immobilization may not be necessary for certain postoperative indications. For instance, in comparative effectiveness studies after ACDF, clinical outcomes show no significant differences in the absence of a hard collar [21–23].
Among the reviewed reports, a prevailing agreement suggests that implant displacement is primarily associated with implant misplacement and/or inadequate fixation. In a study examining 8,887 cases, Smith et al. [23] identified 11 instances of implant extrusion. They linked these cases to the utilization of long complex constructs spanning three or more levels, particularly at the cervicothoracic junction. This specific location subjects the implants to heightened stresses, leading to biomechanical failure [24].
In our case, we suspect that the implant failure occurred during the later postoperative period (2 months after surgery). In hindsight, while there was no apparent instability initially, it is possible that this instability was not evident in the initial dynamic X-ray or that it developed subsequently, resulting in repetitive micro-movements at the injured site.
Also, considering the patient's advanced age, factors such as poor bone quality, facet degeneration, and adjacent segment degeneration may also have contributed to the implant failure.
The cervical collar may have been ineffective in preventing this. This likely contributed to motion at the bone-implant interface, leading to instability, screw loosening, and eventual extrusion. It remains unclear whether the patient was immobilized with a cervical collar in the postoperative period.
This case report underscores the significance of radiographic monitoring. Given the absence of abnormalities immediately after the surgery and the lack of occurrence or worsening of symptoms until the second month post-operation, the issue could not have been identified without the aid of X-ray imaging. Furthermore, when performing ACDF in cervical trauma patients, it is advisable to consider the use of a large size cage or exercise caution with rigid fixation.
The presented case is unique due to the rare occurrence of cage device extrusion in a posterior direction with vertical rotation, while maintaining spinal stabilization and canal space. ACDF cage extrusion is exceptionally uncommon, with an estimated incidence of less than 1% [24]. Similar cases have been reported in the literature during the authors’ extensive review, although not identical in nature.
Conclusion
Cage dislodgement following ACDF is a rare but potential postoperative complication, often associated with fixation failure and spondylolisthesis. There may be hidden issues that are not obvious in the initial state. We recommend minimizing reliance on cervical collars. Regular X-rays are essential for routine follow-up of post-surgical ACDF patients, particularly those with traumatic cervical injuries.
If cage dislodgment and spondylolisthesis occur without symptom deterioration and minimal impact on the spinal canal, close observation can be preferred over immediate additional surgery.
Notes
No potential conflict of interest relevant to this article was reported.