


Introduction
The ossification of posterior longitudinal ligament (OPLL) is a multifactorial disease made by abnormal bone formation that serves to replace spinal ligamentous tissue [1-5]. There are no established facts about the exact cause or mechanism of OPLL [6]. When OPLL develops, it narrows the spinal canal, causing damage to the spinal cord. As a result, patients show clinical symptoms of myelopathy that seriously deteriorate the quality of life [7].
Until now, no studies have investigated the direct connection between ischemic stroke and OPLL. However, ischemic stroke which is a serious disease with functional impairment is related with factors such as infection and atherosclerosis. Through our nationwide longitudinal study, we tried to reveal the association between ischemic stroke and OPLL. We also tried to clarify OPLL increases the incidence of ischemic stroke.
Material and Method
Data source
In South Korea, there is a form of universal health insurance that covers essential medical expenses for all residents under a single public scheme, National Health Insurance Service (NHIS). NHIS provides a general health examination for full time and temporary workers above the age of 40 every year or every two years. It also collects individual data including medical examination with demographic characteristics in the National Health Information Database (NHID). For our study, we have lawfully obtained the right to access the NHID health examination data from 2004 to 2015 with help of the Institutional Review Boards (IRB No. 2020-01-011) of the CHA Bundang Medical Center [8].
Establishment of the study cohort
The total number of 514,557 subjects subjects underwent national health examination and were followed for 12 years until December 31, 2015. The patients with International Classification of Diseases 10th Revision (ICD-10) codes, ‘M48.8, M48.80, M48.81, M48.82, M48.83’, were selected as the OPLL patients (n=3,405). Among those patients, 1,977 subjects are excluded due to lack of computed tomography data. Ones newly diagnosed with OPLL after January 1, 2003 in the remaining group of 1,428 subjects were selected as primary cohorts for our study, which amounted to a total of 1,289. With the ‘Match IT’ R package algorithm, 6,445 subjects were enrolled for the controls through 1:5 age- and sex- stratified matching (Fig. 1). The subjects of the study were followed from the initial date of ischemic stroke diagnosis until their death or the end of the observation period. The occurrence of ischemic stroke was analyzed after controlling age, sex, income, and underlying diseases.
Statistical analysis
Both chi-square test and Student’s t-test were utilized to contrast the demographic factors between the OPLL group and the control group. The Kaplan-Meier method was used to estimate the Ischemic Stroke-free survival probability in each group. Multivariate analysis of the Cox proportional-hazards regression model was used for searching the impact of OPLL on the occurrence of the ischemic stroke. In detail, we made two corrected models, in which model 1 was adjusted for age and sex and model 2 was adjusted for age, sex, income, and medical factors including hypertension, diabetes, and dyslipidemia as covariates. The Cox proportional-hazards regression model and R software version 3.3.3 were used for subgroup analyzes to adjust covariates.
Results
Characteristics of the OPLL and control groups
For the newly diagnosed OPLL group and control group, more part of the subjects were female (51.7%) and an average age was 57.4±9.65 (years). There were some factors which showed significant difference between two groups. One is the diabetes mellitus which has a higher prevalence in the control group (13.0%) than in the experimental group (9.9%; P=0.002). In terms of hypertension, the control group (41.8%) had a higher prevalence than the other group (36.5; P<0.001). In respect of the dyslipidemia a higher incidence was observed in the control group (17.4%) than in the OPLL group (14.5%; P=0.013) (Table 1).
Ischemic stroke in the OPLL and control groups
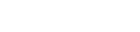
In terms of ischemic stroke, the experimental group (10.687) has a higher incidence rate than the control group (2.011), expressing 1,000 person-year as a unit. Also we found out that its hazard ratio was 4.692 (95% confidence interval [CI], 3.610-6.099) compared to the control group in model 1. In model 2, it was 5.008 (95% CI, 3.845-6.516) (Table 2). In the Fig. 2, when follow-up for ischemic stroke was carried out for 12 years, the cumulative incidence of the experimental group showed a higher number than that of the control group.
Subgroup analysis of the OPLL incidence rate
There are ten subgroups in respect to gender, age, diabetes mellitus, hypertension, and dyslipidemia (Table 3). For all subgroup factors, the incidence rate of ischemic stroke was different between OPLL group and control group. Regarding the incidence of ischemic stroke, there was difference in both male (95% CI, 2.948-6.174) and female (95% CI, 3.724-7.891). There was also significantly deference in age <65 group (95% CI, 4.219-9.111), age ≥65 group (95% CI, 2.538-5.227), non-diabetes mellitus (95% CI, 3.722-6.627), diabetes mellitus (95% CI, 2.376-8.409), non-hypertension (95% CI, 3.591-7.888), and hypertension (95% CI, 3.298-6.694). Lastly, significantly different incidence of ischemic stroke could be observed in both non-dyslipidemia (95% CI, 3.682-6.643) and dyslipidemia (95% CI, 2.425-7.769).
Discussion
Our countrywide longitudinal research found that the OPLL group had 4.692 fold greater incidence of ischemic stroke after controlling sex and age. The OPLL group also had 5.008 fold greater incidence of ischemic stroke after controlling sex, age, wealth, hypertension, dyslipidemia, and diabetes mellitus. In addition, our study showed that the incidence of ischemic stroke was greater in the OPLL group than in the control group in sex, age, non-diabetes, diabetes, non-hypertension, hypertension, non-dyslipidemia, and dyslipidemia subgroups.
Until now, no studies have examined the direct connection between OPLL and ischemic stroke. Instead, several papers have shown that cytokines and inflammation are associated with ischemic stroke. Toma and McCaffrey [9] reported transforming growth factor-β (TGF-β) plays a major role in creating atherosclerosis of blood vessel. It prompts the chemotaxis of repair tissue cells, regulates immunity, and leads to matrix proliferation. Also it negatively regulates antiproliferative processing and apoptotic effects [10-12]. The atherosclerosis of blood vessel can make a thrombosis or block vessels, which leads to ischemic stroke [13-15]. In the development of OPLL, several genes such as TGF-β and bone morphogenetic protein (BMP) are involved. TGF-β/BMP signaling regulates the processing necessary for osteoblastogenesis that promotes progression of OPLL [5]. Thus, this cytokine TGF-β could explain a connection between OPLL and ischemic stroke.
Secondly, Lindsberg and Grau [16] reported systemic markers of inflammation such as the high leukocyte count, fibrinogen, and C-reactive protein (CRP) have been shown to be risk markers of the ischemic stroke. This is because these markers serve as an indication of acute or chronic infectious status. In the infectious tissue, many inflammatory cells secrete inflammatory cytokines into the blood that promote the formation of atherosclerosis and atherosclerotic plaque [4,16-21], which creates thrombosis and increases the risk of ischemic stroke. In addition, Kawaguchi et al. [22] reported a statistical difference in the CRP concentration between the OPLL patients and the non-OPLL patients. The mean serum CRP concentration was 0.122±0.141 mg/dL in the OPLL group and 0.086±0.114 mg/dL in the other group (P=0.047). This means that the CRP concentration was significantly greater in the OPLL patients, so acute or chronic infectious state can indicate a relationship between OPLL and ischemic stroke.
The limitations of our longitudinal cohort study are as follows. First, although our analysis adjusted for sex, age, income, hypertension, diabetes, and dyslipidemia aspects of subjects, our study did not consider the impact of patients’ lifestyle, including the degree of smoking, drinking, exercising, and obesity status. These lifestyle factors may have a crucial impact on the occurrence of ischemic stroke. Secondly, the NHIS database did not have enough information on biomarkers that are related to inflammatory. As a result, it is difficult to understand the exact relationship between OPLL and ischemic stroke through inflammatory markers. Nevertheless, this is the first study attempting to find the connection between ischemic stroke and OPLL in Korean patients. Also it is the largest nationwide longitudinal study indicating an increased risk of ischemic stroke in OPLL patients.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






