


Introduction
Vertebral compression fractures affect approximately 25% of all elderly women [1]. The prevalence steadily increases with advancing age, and especially reaches up to 40 percent in women 80 years of age [2]. Female patients that were diagnosed with a vertebral fracture have a 15% higher mortality rate compared to patients that were not diagnosed [3]. Although less common in elderly men, compression fractures are also major health problems in this group [4-6]. As the proportion of the elderly over 65 years of age in population increases, the incidence of this age-specific fracture is also likely to increase.
Although low bone mineral density (BMD) is considered a typical risk factor for vertebral compression fractures other factors besides BMD are also considered important alongside recently. Loss of muscle mass and sarcopenia have been reported as independent risk factors [7,8]. Studies in respect to sarcopenia have shown that sarcopenia of the extremities is associated with osteoporosis [9]. Because osteoporosis is an important risk factor for sarcopenia, sarcopenia and osteoporosis tend to share common risk factors and biological pathways [10]. Accordingly, interest in the relationship between sarcopenia and vertebral compression fractures has also been ascending.
Hand grip strength (HGS), a measure of voluntary muscle function, has often been used as an indicator of muscle strength. The predictive value of HGS for nutritional status and sarcopenia has been substantiated in a growing number of studies [11,12]. HGS is easy and quick to perform, does not require expensive or complicated equipment, and is a non-invasive test. Therefore, the purpose of our study was to determine the correlation between HGS and vertebral compression fractures in geriatric patient, and to examine the relationship between several other related factors.
Material and Method
Subjects
From March 2018 to December 2021, we retrospectively enrolled vertebral compression fracture patients who were admitted to our general hospital. This study was approved by the Institutional Review Board of Bundang Jesaeng General Hospital (IRB no. 2022-06-002).
Study population
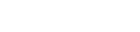
The total of 160 consecutive patients over the ages of 65 years, the World Health Organization standard for the elderly, were included in the study. All patients underwent imaging tests before and after admission. Magnetic resonance imaging (MRI), X-ray, and Computed tomography were included in the imaging examination, and the patients were diagnosed with a vertebral compression fracture accordingly to the consultation of a radiologist. The exclusion criteria were as follows: (1) presence of any other upper spinal disease such as cervical myelopathy, (2) severe pain in shoulder, elbow, hand and finger, (3) peripheral vascular disease, (4) neuromuscular disease, (5) serious medical condition such as stroke or malignancy that can cause disability, (6) inability to complete the questionnaires on health-related quality of life and disability, and (7) transfer to another department without follow up.
Accordingly to these criteria, of the 160 initially included patients, 44 people were excluded, including 38 who met the above exclusion criteria and 6 who refused to participate. Finally, 116 were enrolled in this study. The screening of the study, the inclusion and exclusion flow chart is presented in Fig. 1.
Data collection
Other basic demographic data included gender, age, hypertension (HTN), diabetes mellitus (DM), cardiovascular disease, chronic obstructive pulmonary disease (COPD), rheumatoid arthritis (RA), chronic kidney disease (CKD), and BMD. Body mass index (BMI) was derived from the retrieved height and weight data (BMI=weight (kg)/height2 (m2)). The number of fractured bones was counted through MRI (Achieva; Philips Medical System, Best, The Netherlands), and the frequency of fractures was confirmed through past history taking. The length of hospital stay was also included in the data.
HGS measurement and classification to several groups
HGS was routinely measured for patients admitted to our department with vertebral compression fracture. It was measured for both hands using a dynamometer (EH101; Camry, El Monte, CA, USA, Fig. 2).
The patients sat in a comfortable position, extended their elbows to sides, and then squeezed the dynamometer with maximum force. This test was measured twice with both hands alternately. A small break was taken between each measurement. The highest values of
the repeated measurements were used in the analysis [13]. Regardless of the side and dominance of the hand used as a diagnostic assessment for sarcopenia, the values <26 kg for men and <18 kg for women were used to define sarcopenia according to the guidelines set by the Asian Working Group for Sarcopenia [9,11]. The patients were divided into 2 groups according to the cutoff values, high HSG group (ā„26 kg for men and ā„18 kg for women) or low-HGS group (<26 kg for men and <18 kg for women).
Statistical analysis
Data were presented as descriptive statistics (meanĀ±standard deviation [SD]). Age, BMI and BMD were analyzed by partial correlation to evaluate association of dependent variables. Pearsonās correlation analyses were performed to evaluate the association of dependent variables. Comorbidities such as HTN, DM, cardiovascular disease, COPD, RA, CKD, number of fractured bones, frequency of fractures, and hospital stays were also analyzed. Categorical variables were analyzed using the chi-square test, whereas continuous variables were analyzed using independent t- test to evaluate the differences between groups classified according to the HGS values. Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows ver. 21.0; IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Statistical significance was defined as P<0.05.
Results
Clinical characteristics of the participants
During the study period, 116 subjects with vertebral compression fracture were enrolled. The participants were comprised of 35 males, 81 females with a mean age of 76.30Ā±12.01 years. In terms of the underlying disease group, there were 36 HTN patients, 32 DM patients, 26 cardiovascular disease patients, 9 COPD patients, 14 CKD patients, and 12 RA patients. The mean BMI was 23.25Ā±4.23 kg/m2, the mean BMD was -2.73Ā±1.31, and the number of fractured bones were classified as 1, 2, 3, 4 or more. Accordingly, to the total number of previous compression fractures, patients were classified into once, twice, three times and more than three times. The length of hospital stay was 14.47Ā±9.87 days. The demographic characteristics of 116 participants are summarized in Table 1.
Analysis of other clinical parameters between the different HGS groups in patients with compression fracture
Chi-square test and independent t-test were performed. The result of analysis between HGS groups and other clinical parameters are presented in Table 3. Clinical parameters include patientsā comorbidities and other parameters.
Chi-square test revealed that CKD (P=0.031) and RA (P=0.024) were significantly different between 2 groups. HTN, DM, and cardiovascular disease were also statistically analyzed, but there was no significant relationship with HGS groups.
Independent t-test revealed that there were significant differences in the number of fractured bones and frequency of fractures between the 2 groups. The number of fractured bones (meanĀ±SD) of the low-HGS group (1.78Ā±0.31) was significantly larger than that of the high-HGS group (1.28Ā±0.19, P=0.021). The frequency of fractures (meanĀ±SD) of the low-HGS group (1.60Ā±0.22) was also significantly larger than that of the high-HGS group (1.15Ā±0.24, P=0.017). The length of hospital stay had no significant difference between the 2 groups.
Discussion
The purpose of this study was to investigate the HGS of elderly patients with compression vertebra fractures and to evaluate the association between HGS and other factors.
The study results showed that HGS was strongly associated with the frequency and numbers of compression fractures. The number of fractured bones of the low-HGS group representing sarcopenia was significantly larger than that of the high-HGS group. Our analysis showed the same results in the frequency of fractures.
The current consensus regarding the definition of sarcopenia is the presence of both low muscle mass and low muscle function (strength or performance) [11,14]. HGS is commonly used to measure voluntary muscle function as an indicator of muscle strength. Sarcopenia in patients with osteoporotic fractures has been documented regularly [15]. Osteoporosis is importantly related to sarcopenia in elderly populations [10]. Sirola et al. [16] reported that good muscle strength and its maintenance are associated with higher BMD and lower bone loss rate. In our study, HGS and BMD showed a strong correlation. The group with low HGS had more osteopenia and osteoporosis patients, and the group with high HGS had fewer osteopenia and osteoporosis patients. As mentioned above, osteoporosis is an important risk factor for the vertebral compression fracture in elderly [10]. This supports our findings regarding the relationship between HGS and compression fractures.
Our study also showed that RA and CKD are possible related factors. RA and CKD are representative chronic inflammatory diseases that not only cause joint and bone destruction, but also affect the loss of muscle volume and strength [17]. One study documented that, normal body weight with RA, the adjusted odd ratio (OR), the loss of lean body mass was more than 3 times greater (OR, 3.41; P<0.05) than in the control group [18]. Meanwhile, kidney disease can cause muscle wasting through accelerated muscle protein breakdown, which may be possibly mediated by mitochondrial respiratory dysfunction or reduced muscle mitochondrial mass [19].
There was no significant difference in BMI and the length of hospital day from the results of the demographic analysis. Shen et al. [20] reported a significant difference in BMI between high and low-HGS groups. However, because the data of men and women were not separated in this study, the body mass of subjects would differ according to the proportion of men and women. In addition to the patientsā pathological factors, the length of hospital days depends on several other factors. In the case of elderly patients, not only the length of hospital stays due to fractures, but also many underlying diseases have also affected the length of hospital stays [21].
The strengths of this study include the use of HGS measurement, which is a very simple test that can represent sarcopenia. The relationship between HGS and vertebral compression fracture can be seen. However, our study had several limitations. This was a retrospective single-center study with a relatively small sample size. Larger study is necessary to reach a solid conclusion on the relationship between HGS and vertebral compression fracture. In addition, more linking variables, such as lean body mass or muscle volume from imaging studies, could be used for patient evaluation.
In conclusion, this is the first study that evaluated the several factors associated with HGS in elderly patients with vertebral compression fracture. Our result reveals that the Hugh and low of HGS in geriatrics is significantly associated with number of fractured bones and frequency of fractures, and that BMD, RA, CKD can be the possible associated factors.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






