


Introduction
The prevalence of degenerative diseases, such as osteoporosis, muscle degeneration, and degenerative spine disease, is high in the elderly. In addition, the aging population is rapidly increasing, and the incidence of osteoporosis and degenerative diseases is increasing along with it. Osteoporosis is characterized by bone microarchitecture destruction and bone quality degradation [1], leading to decreased bone strength due to decreased bone mineral density (BMD) or poor bone quality. Osteoporotic fractures can occur easily with minor trauma or even without any noticeable trauma in these patients [2]. However, elderly patients with degenerative diseases may develop vertebral compression fracture (VCF), with or without osteoporosis. VCF affects quality of life, daily activities, and mortality in elderly patients [3]. In South Korea, the 5-year incidence of osteoporotic VCF per 100,000 persons is 852.24 cases, and 45% of osteoporotic VCF cases occur in patients over 70 years of age. Moreover, vertebral body cement augmentation or any surgical approach rate and total cost related to VCF are increasing [4].
Patients with VCF are treated with conservative care with bed rest and bracing. Conservative care generally has a good outcome. However, some VCF patients have severe vertebral body height loss and fractured bony fragment compression of the spinal cord or thecal sac. VCF progression can result in neurological deficits and spinal deformity, in which patients experience reduced daily activities, prolonged severe back pain, and reduced quality of life. In this case, surgical treatment is subsequently required.
Therefore, it is important to predict and prevent the progression of VCF. Previous studies have focused on VCF progression and have analyzed vertebral body fracture shape, presence of an intravertebral cleft, posterior wall damage, middle column damage, and VCF progression [5,6]. However, few studies have investigated the association between spinal muscle fatty degeneration and VCF progression, which were published only recently [7,8]. Therefore, our study is an additional study on the association between spinal muscles fatty degeneration, functional support of the spinal muscles, and VCF progression.
Material and Method
The study protocol was approved by the Institutional Review Board of Inje University Haeundae Paik Hospital (IRB no.2022-05-024). The requirement for informed consent was waived owing to the retrospective nature of this study. We retrospectively evaluated 186 consecutive elderly patients over 65 years of age who had VCFs between 2013 and 2020. Patients who was examined lumbar magnetic resonance imaging (MRI) and follow-up X-ray were selected. VCF levels were limited to thoracolumbar and lumbar lesions. Patients with BMD and osteoporosis were also included. The exclusion criteria were as follows: (1) no MRI performed, (2) no follow-up X-ray image (>6 months) and (3) image could not be evaluated. In total, 49 patients were enrolled in this study.
Radiological parameters
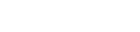
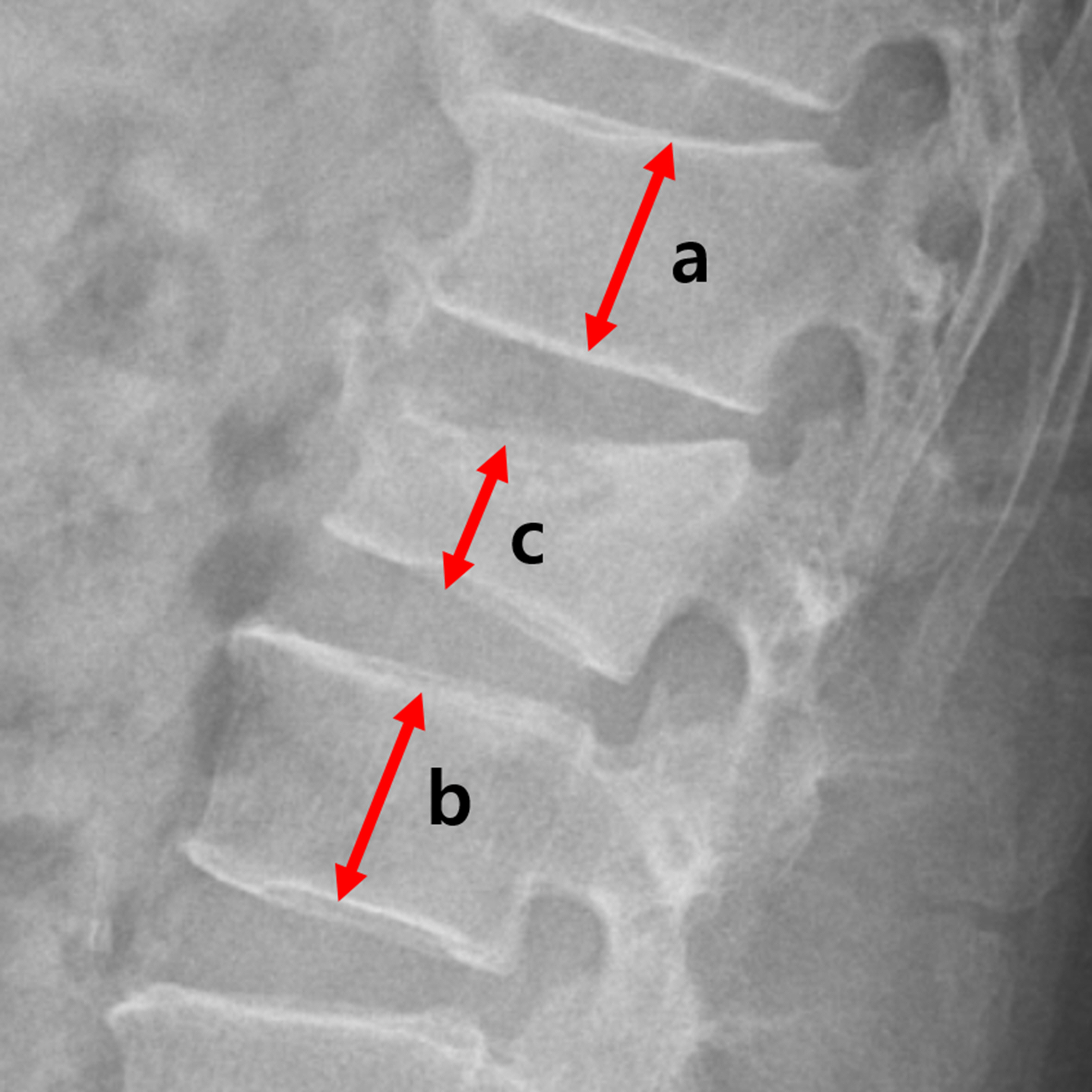
All patients underwent plain X-ray and MRI. Sagittal plain X-ray was obtained for the initial VCF, first follow-up X-ray image one weeks later and at 1, 3, and >6 months. MRI was performed during hospitalization after VCF onset. VCF height loss was measured as the point of maximal collapse of the affected vertebral body; vertebral collapse (%) was measured using the formula {(upper vertebral height+lower vertebral height)/2-(affected vertebral height)/(upper vertebral height+lower vertebral height)/2}├Ś100 (Fig. 1) [9]. Change in height loss was defined as difference in height loss in vertebral collapse between the initial and >6-month follow-up. Fatty infiltration of the paraspinal and psoas muscles was measured using T2-weighted MRI at L3 and L4. We used the open-source software ImageJ (ver. 1.53 k, Wayne Rasband, National Institutes of Health, Bethesda, MD, USA). Fatty infiltration of the multifidus, erect spinae, and psoas muscle were determined by measuring the cross-sectional area (CSA) of the muscles in T2-weighted MRI using the threshold grayscale in ImageJ (Fig. 2) [7,8]. The paraspinal muscle mass, excluding fat, was calculated by multiplying the ratio of fat by the simple area of the paraspinal muscle. The actual paraspinal muscle mass was measured using the following formula {CSA of the paraspinal muscleŌłÆ[paraspinal muscle fat ratio (%)├ŚCSA of the paraspinal muscle (mm2)]}. We evaluated all methods used previously was applied to measure the psoas muscle mass. The paraspinal muscle to psoas muscle mass ratio was measured using the formula (CSA of the paraspinal muscle/CSA of the psoas muscle).
Statistical analysis
All statistical analyzes were performed using R ver. 4.1.2. A 2-sample t-test was performed for continuous variables that satisfied covariance. WelchŌĆÖs 2-sample t-test was performed for continuous variables that did not satisfy covariance. Logistic regression analysis was performed for categorical and continuous variables. Stepwise logistic regression analysis was performed using backward elimination. Odds ratios (ORs) between the related factors were calculated. Statistical significance was set at a P-value of <0.05.
Results
Patient characteristics and radiological parameters
The average age of the 49 patients was 79.12┬▒8.59 years, and there were 30 female and 19 male patients. BMD was ŌłÆ2.02┬▒1.87. Body mass index (BMI) was 23.65┬▒2.00 kg/m2. The follow-up VCF height loss change was 6.53┬▒4.90 mm. The CSA of the paraspinal muscle was 2,418.00┬▒496.00 mm2. Fatty infiltration rate of the paraspinal muscle was 4.46%┬▒1.70%. The CSA of the psoas muscle was 962.00┬▒351.00 mm2. Fatty infiltration rate of the psoas muscle was 1.00%┬▒0.50%. The revised paraspinal muscle is a value obtained by subtracting the fatty infiltration area from the CSA of the paraspinal muscle area. The revised paraspinal muscle was 2,310.00┬▒481.00 mm2. The paraspinal-to-psoas muscle mass ratio was 2.73┬▒0.82. Sixteen patients required surgical procedures, including posterolateral fusion in 3 cases, corpectomy with posterior pedicle screw insertion in 2 cases, and vertebroplasty in 11 cases. The mean number of cases that received osteoporosis medications was 20 (Table 1).
Relationship between VCF height loss progression and fatty infiltration of the paraspinal and psoas muscle
The mild VCF height loss group (n=36, group 0) included cases of VCF height loss change of Ōēż9 mm, and the severe height loss group (n=13, group 1) included cases of VCF height loss change of >9 mm. The groups were divided using the mean and standard deviation of height loss in all cases. The paraspinal-to-psoas muscle ratio was 2.51 in group 0 and 3.33 in group 1 (P=0.002). The CSA of fatty infiltration of the paraspinal muscle was 102.17 mm2 for group 0 and 121.96 mm2 for group 1 (P=0.28). The paraspinal muscle mass was 2,383.63 mm2 in group 0 and 2,512.07 mm2 in group 1 (P=0.43). The revised paraspinal muscle [CSA paraspinal muscle (mm2)├ŚParaspinal muscle fat infiltration(%)ŌłÆCSA Psoas muscle (mm2)├ŚPsoas muscle fat infiltration (%)] was 2,281.46 mm2 in group 0 and 2,390.11 mm2 in group 1 (P=0.49). The revised psoas muscle was 1,004.8 mm2 in group 0 and 844.80 mm2 in group 1 (P=0.16) (Table 2).
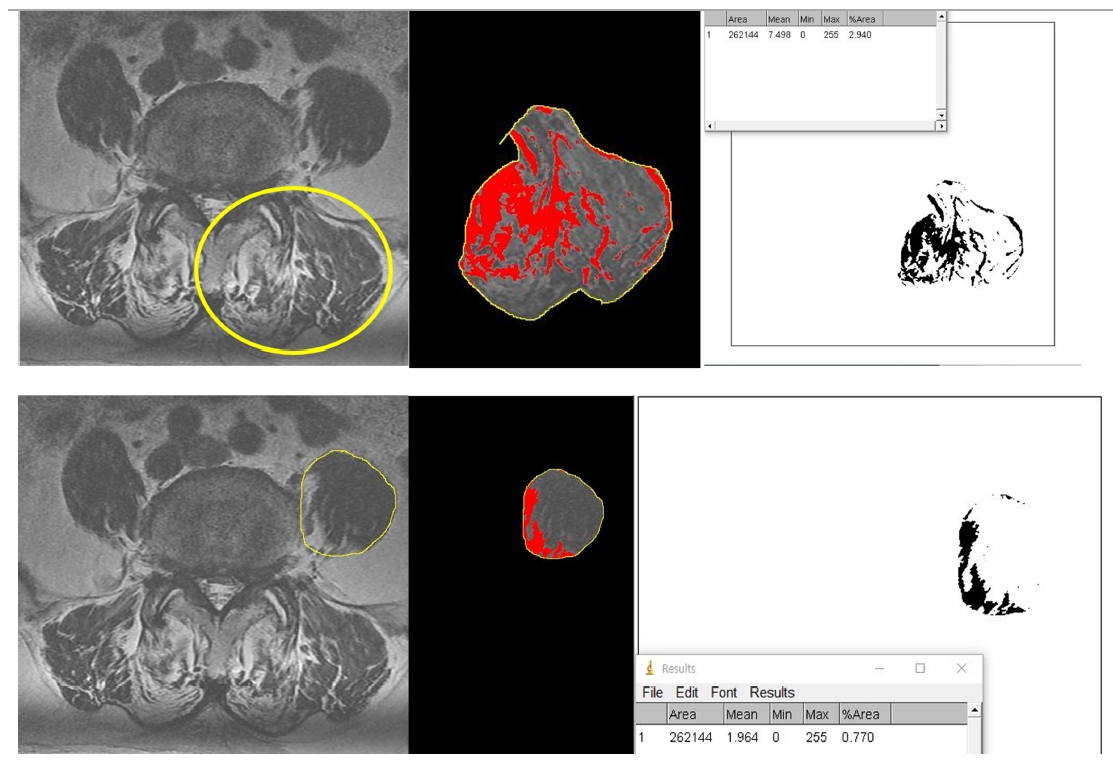
Logistic regression was performed to verify the relationship between the number of radiological factors and VCF height loss changes. The paraspinal-to-psoas muscle ratio showed an OR,13.42; 95% confidence interval (CI), 0.75ŌłÆ882.90; P=0.10, fatty infiltration of the paraspinal muscle had an OR, 0.17; 95% CI, 0ŌłÆ4.8; P=0.30, and BMD showed a negative relationship with an OR, 0.50; 95% CI, 0.18ŌłÆ1.10; P=0.10). Stepwise logistic regression analysis was performed using backward elimination. The paraspinal muscle mass (P=0.02), BMD (P=0.05), and paraspinal-to-psoas muscle mass ratio (P=0.01) remained unchanged. The OR of the paraspinal-to-psoas muscle ratio was OR, 4.39; 95% CI, 1.32ŌłÆ14.56 (P=0.01). However, the paraspinal muscle OR was 1, which did not significantly affect the results. (Table 3, Fig. 3)
Discussion
Muscle degeneration is associated with an increased risk of bone fracture and difficulty in performing daily living activities. Sarcopenia is the loss of muscle mass associated with aging and advanced disease. It has previously been shown to predict complications and mortality in patients undergoing emergency surgery, surgical oncology, and organ transplantation [10-12].
VCF has a high prevalence in older patients, and VCF height loss change greatly reduces their quality of life. The paraspinal and psoas muscles are expected to influence VCF progression. Bayram et al. [13] previously reported that psoas muscle degeneration was associated with mortality in VCF patients using the psoas muscle:lumbar vertebral index. Although no statistical significance was observed in this study, group 1 (severe VCF height loss) showed lower psoas muscle mass. In addition, Bokshan et al. [14] reported that L4 total psoas muscle sarcopenia increased postoperative morbidity in patients who underwent spine surgery.
Paraspinal muscles have a major impact on the maintenance of spinal alignment. Thus, paraspinal muscle atrophy, fatty infiltration, and degeneration affect the spinal sagittal balance and global alignment [15,16]. The relationship between paraspinal muscle and lumbar pathology has been reported in previous studies. Jun et al. [15] reported that fatty infiltration of the paraspinal muscles was significantly negatively correlated with the thoracolumbar curve. Habibi et al. [17] reported that fatty infiltration of the paraspinal muscle in the thoracolumbar region is correlated with the occurrence of new osteoporotic VCF. Katsu et al. [18] reported that the erect spinal muscle has a marked influence on fracture union of the VCF. However, Osterhoff et al. [7] reported that the multifidus area and fatty infiltration had no significant effect on the occurrence of adjacent vertebral fractures within 1 year of the index fracture. In addition, the paraspinal muscle does not affect vertebral collapse but the revised paraspinal muscle does. The paraspinal muscle affects functional movement and stability of the vertebral column [19,20]. In this study, the paraspinal muscle mass was greater in group 1, but fatty infiltration showed a higher average in group 1, regardless of muscle mass. However, the difference was not statistically significant. Moreover, it was difficult to determine the relationship with paraspinal muscle VCF progression, even when logistic regression was performed.
Therefore, in this study, unlike previous studies that independently studied the psoas and paraspinal muscles, we investigated how the relationship between the degeneration of the 2 muscles affects VCF progression. As a result, the paraspinal-to-psoas muscle ratio was higher in group 1. This suggests that degeneration in the psoas muscle is more associated with VCF progression than that in the paraspinal muscle. In addition, when logistic regression analysis with various factors was performed, the paraspinal-to-psoas muscle ratio (P=0.05) showed the greatest correlation with the OR of 4.39. Many studies have independently investigated the paraspinal and psoas muscles, but ours is the first to report on the relationship between the 2 muscles, and as such, there has not been a study on the cause of VCF progression in a group with a large paraspinal-to-psoas muscle ratio. With respect to muscle function, the psoas muscle affects the bipedal walking function [21]. In group 1, with a large paraspinal-to-psoas muscle ratio, bipedal walking function further decreases and muscle fatigue occurs because of the small size of the functional muscle mass when standing or walking. So group 1 patient should be need a more absolute bed resting and early bed side rehabilitation for psoas muscle and paraspinal muscle. During in hospitalization, if group 1 patient low back pain will not improve, it may be a sign that there is no bone union in the vertebral body [8].
This study had several limitations. First, the sample size was small. Further research based on additional cases in follow-up studies is required. Second, muscle mass and fatty infiltration were assessed using images at specific time points. MRI obtained at regular intervals would have resulted in better results. Third, there may have been errors during measurement. Because millimeter is a very small and sensitive unit, there may have been errors during measurement.
Conclusion
In this study, the associations between BMI, BMD, paraspinal muscle, psoas muscle, muscle fatty infiltration, paraspinal-to-psoas muscle ratio, and VCF progression were analyzed. Among the various factors, the paraspinal-psoas muscle ratio strongly influences VCF progression. In patients with VCF, VCF progression can be predicted using the paraspinal-to-psoas muscle ratio before ambulation.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






