


Introduction
Cerebellar infarcts are medically curable diseases, and the majority of patients show mild symptoms, such as dizziness, vertigo, and ataxia [1]. However, a subgroup of patients with severe cerebellar swelling show clinical or radiological deterioration within several days after the onset of cerebellar stroke. Large cerebellar infarctions can result in a space-occupying mass effect and increase posterior fossa pressure. This pathophysiologic phenomenon can cause critical complications such as obstructive hydrocephalus, brain stem compression, and upward transtentorial herniation or downward transforaminal herniation, ultimately resulting in life-threatening conditions [2-5].
Surgical treatment is essential in patients who show severe neurological deterioration despite receiving maximal medical therapy. External ventricular drainage (EVD) is considered to be the first step in surgical management and is recommended for the treatment of obstructive hydrocephalus after cerebellar infarction [6]. In patients with cerebellar infarction showing clinical deterioration due to severe swelling, decompressive suboccipital craniectomy (DSC) with dural expansion is recommended as a life-saving procedure [6-9]. In each case, necrosectomy and/or resection of the posterior arch of C1 was performed additionally, and some previous studies have described their therapeutic effects [4,10,11].
However, long-term follow-up data of DSC are insufficient, with some debates on the optimal surgical technique, timing of surgery, and prognostic factors [7,8,12]. In our retrospective study, we surgically treated 33 patients with cerebellar infarction accompanying massive cerebellar swelling. We also analyzed the long-term outcomes and prognostic factors of decompressive surgery in patients with severe cerebellar infarction.
Material and Method
Patient selection
The study was designed as a retrospective, single-center trial. We included consecutive patients with cerebellar infarction accompanied by severe cerebellar swelling treated by DSC from January 2008 to December 2018. Additional procedures such as EVD and necrosectomy were performed if deemed appropriate. Data pertaining to the patients’ medical history, neurological evaluation, radiological examinations, and surgical treatment were obtained from computerized patient charts. Patients with insufficient follow-up data were excluded from the study. A total of 33 patients who underwent DSC for cerebellar infarction were included in the study. The investigative protocol was approved by Inje University's Institutional Review Board (no. 2021-05-009).
Radiological evaluations
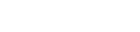
Brain computed tomography (CT) was initially performed for diagnosis, and brain magnetic resonance imaging (MRI) was conducted to confirm cerebellar infarction. In some cases, digital subtraction angiography was performed to confirm the arteries involved and to exclude abnormal vascular lesions. A neuroradiologist who was not involved in the treatment rated the mass effect on brain swelling caused by cerebellar infarction by assessing preoperative brain CT images according to the CT score published by Jauss et al. [13]. This scoring system evaluates the ventricle, quadrigeminal cisterns, and lateral ventricle, and each item is graded from 0 to 3 depending on the severity. The total score was calculated by adding the scores for each item. A total score of 0 to 3 indicated no or slight mass effect, 4 to 6 indicated a moderate mass effect, and 7 to 9 indicated a severe mass effect (Fig. 1).
Surgical procedure
We performed decompressive surgery and maximal duraplasty in patients with moderate to severe cerebellar swelling who showed acute neurologic deterioration despite maximal medical therapy. The CT scores were used to recognize infarct size and degree of brainstem compression, but the swelling and mass effects may deteriorate quickly in the acute period, so we gave more importance to the immediate symptoms of patients in determining surgery. Removal of necrotic tissue and resection of the posterior arch of C1 could be determined by CT findings prior to surgery, but were mostly determined by the degree of brain swelling in the surgical findings. EVD was performed in the right frontal horn if compression of the fourth ventricle with obstructive hydrocephalus was apparent before or after DSC.
Examination protocol
All patients were treated in the neurological intensive care unit (NICU), examined using a standardized examination protocol, and evaluated in serial neurological examinations conducted daily after hospitalization and immediately before and after surgery. The level of consciousness was assessed using the Glasgow coma scale (GCS). We also assessed cranial nerve abnormalities and focal neurological signs, including motor abnormalities, coordination disturbances, sensory disturbances, and reflex status. Repeat CT was performed at least 3 times during the pre- and postoperative periods. Functional deficits were assessed using the modified Rankin scale (mRS): 1=no symptoms; 2=no significant disability despite mild symptoms; 3=moderate disability, requires some help, but is able to walk without assistance; 4=moderate severe disability, unable to attend to own bodily needs without assistance and unable to walk without assistance; 5=severe disability, requiring constant nursing care, being bedridden; and 6=death. The mRS score was examined at each outpatient visit after discharge.
Analysis and statistical methods
Demographic data, clinical features, level of consciousness evaluated using the GCS, neurological and radiological examination data, and surgical results were obtained from the patients’ electronic medical records. We divided the patients into 2 groups according to the mRS scores measured 2 years after surgery to determine the long-term prognostic factors. Based on previous studies, a mRS score of 4 or more was considered to indicate a poor outcome [14-17]. Age, GCS score before surgery, bilateral infarction, brainstem infarction, surgical methods, and time between stroke onset and DSC were investigated for the analysis of prognostic factors. To compare categorical data between the groups, cross-tables were produced using Fisher exact test to determine statistical significance. The Mann-Whitney U test was used for continuous data. Statistical analysis was performed using IBM SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA), and a P-value <0.05 was considered to indicate significance.
Results
Patient characteristics
Data were collected from 33 patients who underwent DSC for acute cerebellar infarction. Twenty-two patients (66.7%) were male, and the average age was 63 years (range, 43-82 years) (Table 1). Twenty-seven of 33 patients had at least one cardiovascular risk factor, such as atrial fibrillation (2, 6.1%), hypertension (25, 75.8%), diabetes mellitus (10, 30.3%), hypercholesterolemia (6, 18.2%), smoking (10, 30.3%), or chronic kidney disease (1, 3.0%). Before cerebellar infarction, none of the patients suffered brain damage, including cerebral hemorrhage, infarction, or tumors.
Clinical findings and preoperative course
The median GCS score was 13, and 28 patients had a GCS score ≥8 at admission. The most common symptoms of cerebellar infarction onset were vertigo (75.8%) and nausea (39.4%). The most common focal neurological abnormalities at admission were ataxia (72.7%) and decreased consciousness (69.7%). In most patients (30, 90.9%), consciousness deteriorated between admission and surgery, with a median GCS score reduction from 13 to 8. Mean time from stroke onset to surgery was 15.8±17.2 hours (range, 4-72 hours). Twenty-four patients underwent DSC within 24 hours after admission, 7 underwent surgery between 24 and 48 hours after admission, and 2 underwent surgery between 48 and 72 hours after admission.
Neuroradiological findings
Brain CT was performed in all patients, and additional examinations, including CT angiography, MRI, and transfemoral cerebral angiography, were performed to better delineate infarct extension in some patients. Cerebellar infarction was bilateral in 8 patients (24.2%). The territory of the posterior inferior cerebellar artery (PICA) was the most commonly affected (87.9%), followed by the superior cerebellar artery (SCA). Additional brainstem infarctions were found in 7 patients (21.2%) (Table 1). Fourth ventricle compression was found in most patients (28, 84.8%), and hydrocephalus was found in 16 patients (48.5%).
Surgical treatment
All 33 patients were treated with DSC and duraplasty. Removal of necrotic tissue was performed in 10 patients (30.3%). Preoperative EVD was performed in 3 patients to prevent upward transtentorial herniation. Postoperative EVD was performed in 5 patients who showed persistent hydrocephalus after DSC and in one patient with postoperative intraventricular hemorrhage. Seven patients with mild hydrocephalus did not require EVD. Minimal intracerebral hemorrhage was found on postoperative CT in 2 patients, but no additional surgery was required. The EVD could be removed within 2 weeks in all patients, and none of the patients underwent ventriculoperitoneal shunting. None of the patients required resection of the posterior arch of C1.
Early course and mortality
All patients were monitored and treated in the NICU. The mean duration of NICU treatment was 21.3±11.2 days (range, 7-72 days). During this phase, 2 patients died: 1 patient died from acute myocardial infarction and one patient died from sepsis. The surviving patients were referred to the rehabilitation department. One month after discharge, one patient died of myocardial infarction.
Long-term outcome and prognostic factors
Over a follow-up period of approximately 2 years, no other patients died. Twenty-one of the 30 patients had a favorable functional outcome (mRS, 0 to 3), while the remaining 9 patients showed persistent major disability (mRS, 4 to 5) at the 2-year follow-up assessment. Fig. 1 shows the distribution of mRS scores. In univariate analysis, radiological findings of brainstem infarction were associated with poor outcomes (mRS ≥4) at the 2-year follow-up (Table 2). Only 1 of the 21 patients in the favorable functional outcome group showed brain stem infarction, while 4 of the 9 in the poor functional outcome group had brain stem infarction. Patients in the favorable outcome group were younger than those in the poor outcome group on average (60.29 vs. 64.89 years), but the difference was not statistically significant (P=0.33). Other factors such as sex, GCS score, vascular risk factors, etiology, symptoms, surgical factors, CT scores, neurological signs, and the laterality of cerebellar infarction showed no significant association with poor outcomes.
Discussion
DSC is considered the treatment of choice in patients with space-occupying cerebral infarctions [5,7,9,18-21]. However, the surgical procedures for cerebellar infarction are decided on the basis of clinical experience and previous retrospective studies because randomized controlled trials comparing surgery to medical treatment for severe cerebellar infarction are difficult to perform; thus, retrospective studies of long-term prognostic indicators after DSC can be performed to improve the validity and reliability of surgery. Our findings confirm that poor functional outcomes at approximately 2 years after DSC were more related to brain stem infarction than any of the other factors.
Although surgical indications for space-occupying middle cerebral artery infarction have been standardized through randomized controlled trials, the surgical treatment for cerebellar infarction is still not standardized [22-24]. This has led to some debates on the type of surgery, including DSC, EVD, additional necrosectomy, and resection of the posterior arch of C1. This study included no cases of resection of the posterior arch of the C1. EVD was considered the initial treatment for patients showing decreased consciousness due to obstructive hydrocephalus and was performed in patients with persistent hydrocephalus at any time before or after surgery. Additional evacuation of necrotic tissue was performed during DSC in patients who required an increase in decompression volume and decreased cytotoxic edema. Although the use of various surgical methods caused great heterogeneity in the prediction of prognostic factors, the analysis is meaningful because all surgical methods achieved the primary objective of ensuring decompression of the cerebellum to minimize damage to brain tissue.
In this study, the mortality rate was 9.1% (3/33), and 30.0% (9/30) of the patients had poor functional outcomes (mRS ≥4). Previous studies on long-term outcomes have reported mortality rates ranging from 20% to 32%, with 40% to 49% of the patients showing poor outcomes [7-9,18,25,26]. In a systematic review and meta-analysis by Ayling et al. [26] (11 studies with 283 patients), moderate to severe disability was observed in 28% of patients, and the mortality rate at a median follow-up period of 9 years after DSC for cerebellar infarction was 20%. In a study by Lindeskog et al. [18], poor outcomes (mRS ≥4) were seen in 46% of 22 patients at the yearly follow-up after DSC, and brainstem infarction and bilateral cerebellar infarction were associated with poor outcomes. The mortality rate and percentage of patients showing poor outcomes in the present study were lower than those in previous studies. This may be attributed to the short follow-up period (2 years). In addition, the selective bias, in which patients who can visit the hospital often would have affected it.
Decreased level of consciousness with or without brain stem compression signs is a strong indication for decompressive surgery [8,13,27]. Neurological deterioration usually occurs within 3 to 4 days (range, 0-9) after onset [5,8,13,28,29]. Due to the non-specific symptoms of cerebellar infarction and the low sensitivity of CT imaging in evaluating the posterior fossa, edema development is not recognized until it becomes severe. Therefore, deterioration of consciousness is an important warning sign of severe cerebellar swelling [8,13,27]. For immediate treatment, including surgery, patients should be kept under observation in stroke or intensive care units for the first week after onset. Although some studies have shown that preoperative GCS scores are predictors of long-term outcomes [8,16,30], they were not statistically significant in our study. This is presumed to be due to the fact that a number of factors were not controlled, including the time taken to arrive at the hospital and the medication content.
Many authors report that the most frequently affected area in cerebellar infarction is the PICA territory, followed by the SCA [7,31-33]. Some reports have demonstrated that patients with PICA infarction are especially at risk for malignant cerebellar edema, and severe swelling in isolated SCA and anterior inferior cerebellar artery (AICA) infarction is rare [34]. The most commonly affected artery in our study was the PICA, followed by the SCA, PCA, and AICA. A comparison of swelling severity was not possible because data regarding arteries other than the PICA were scarce in our study.
In this study, a high CT score indicating severe compression was not associated with patient prognosis. Rather, the presence of brainstem infarction showed the greatest effect on prognosis. Decompressive surgery can release the brainstem pressure caused by brain swelling; however, the effectiveness of decompression surgery is reduced if the brainstem itself is infarcted. Moreover, this study only focused on patients with severe cerebellar infarction who underwent surgery, so comparison of CT scores with those obtained for patients who received only medical treatment would produce meaningful results. In addition, we recommend preoperative MRI examinations to distinguish brainstem infarction and compression. Since the evaluations and CT scoring were performed just before surgery, moderate grade accounted for the largest percentage of cases (Table 2).
Limitations
This study had several limitations. First, this was a retrospective study that only compared patients who underwent surgery. The exclusion of patients with cerebellar infarction who only received medical treatment caused a selection bias. Second, additional EVD or necrosectomy was performed at the discretion of the 4 surgeons without a standardized protocol. Therefore, this study only reflects the postoperative prognosis of a selected group patients, and the findings have limited generalizability. For this reason, a randomized controlled study with a wider patient population should be conducted to improve the overall quality of the findings, allowing appropriate comparison of the prognosis of different surgical methods.
Conclusion
Surgical treatment is an essential procedure that can save the lives of patients with severe cerebellar infarction. However, surgical protocols are not well-established, and there is a lack of research on the long-term prognostic factors after surgery. Our study showed that the presence of brainstem infarction influenced the postoperative functional outcomes. This finding can facilitate the long-term management of these patients, including rehabilitation for functional recovery. Future research should focus on identifying prognostic factors that can predict functional outcomes by standardizing treatment protocols for severe cerebellar infarction.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






