A novel technique for surgical excision of a symptomatic lumbar spine facet joint synovial cyst using a cyst dyeing method: a report of two cases and a literature review
Article information

Abstract
The aim of this study was to investigate the efficacy of a cyst dyeing technique that was used during the surgical excision of facet joint cysts in 2 cases. We evaluated the patients’ clinical outcomes and perioperative complications after decompression of lumbar spinal stenosis caused by the cysts. Two patients, who underwent surgical decompression for symptomatic lumbar spinal stenosis caused by facet cysts in August and October 2020, were reviewed. Their main complaints were severe low back pain and sciatica 1 or 2 months ago, for which they visited Wooridul Spine Hospital, Daegu, Korea. Under general anesthesia, the cysts were removed with the cyst dyeing method, using indigo carmine. Clinical outcomes were assessed by preoperative and postoperative visual analog scale (VAS) scores. Perioperative complications were observed. Favorable clinical outcomes and no perioperative complications were reported. Low back pain and sciatica improved, as shown by changes of the VAS score from 9 or 8 to 1, and no dural defects were observed. The cyst dyeing method is an effective technique for the surgical removal of symptomatic lumbar spine facet joint cysts.
Introduction
Lumbar spine facet joint synovial cyst is a benign protrusion from facet joint capsules caused by degenerative change. It commonly induces symptoms of low back pain, radiculopathy, neurogenic claudication, and cauda equina syndrome, because it leads to lumbar spinal stenosis and lumbar foraminal stenosis [1].
The treatment of symptomatic lumbar synovial cysts varies widely from surgical excision to conservative treatments. The gold-standard treatment for symptomatic synovial cysts is surgical removal [2–6]. However, this presents unique challenges resulting from adhesion between the cyst and dura mater. The challenges include the identification of clear anatomical boundaries and mechanical separation between the cyst and thecal sac. These characteristics lead to a higher incidence of dural tears during surgery.
Here, we describe surgical excisions using a cyst dyeing method, which involves the injection of indigo carmine into the cyst. The method is a novel attempt. This makes cyst removal easier and safer by clarifying the anatomical boundaries between the cyst and dural sac, facilitating the separation procedure, and preventing dural injury.
Case Report
Case 1
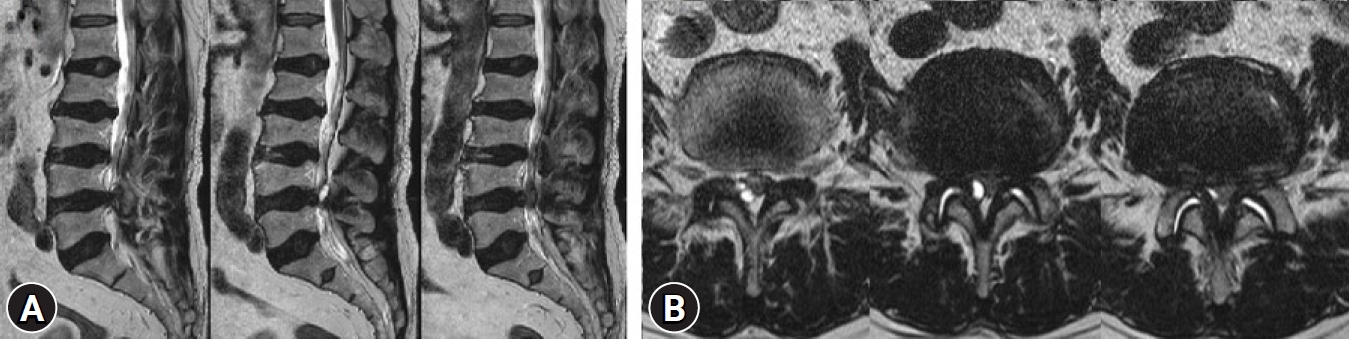
In August 2020, a 76-year-old woman presenting with severe low back pain and left leg radiating pain 1 month ago visited the Wooridul Spine Hospital, Daegu, Korea. The pain was evaluated by a visual analog scale (VAS) score of 9. She could not sleep due to the pain. Magnetic resonance imaging (MRI) demonstrated a L5–S1 facet joint synovial cyst compressing the left S1 nerve root (Fig. 1). After informed consent was obtained from the patient, 2 staged procedures were conducted.

Preoperative images of a lumbar facet joint synovial cyst at the left L5–S1 level on magnetic resonance imaging (MRI). (A) Sagittal image on T2-weighted MRI. (B) Coronal image on T2-weighted MRI.
The first staged procedures were computed tomography guided percutaneous cyst aspiration and transforaminal epidural steroid injection at left S1 nerve root. However, the cyst was not sufficiently aspirated and the symptoms were not resolved.
The second staged procedures were left laminectomy at the L5–S1 level and surgical cyst excision with a cyst dyeing technique. Under general anesthesia, the patient was placed in a prone position. A 20-mm long skin incision was made to target the L5–S1 disc space level. A Caspar retractor and Counter were inserted through the incision. After microscopic left laminectomy at the L5–S1 level, a 6-mm facet joint cyst was observed near the lateral margin of the thecal sac. Then, 1 mL of indigo carmine (180 mg/10 mL, Indigo Carmine; Teva Takeda Pharma Ltd., Nagoya, Japan) was injected into the cyst to identify clear anatomical boundaries between the cyst and dural sac (Fig. 2). We separated the cyst and dura efficiently without dural tearing. The operative time was about 50 minutes. The patient reported improved low back pain and left leg radiating pain, which was represented by a reduction in VAS score from 9 to 1.
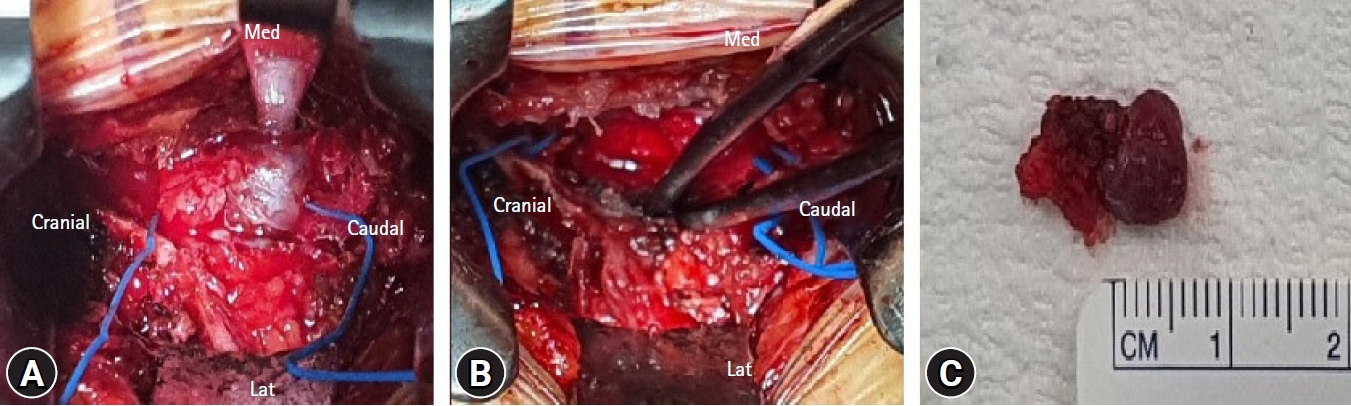
Intraoperative images of surgical excision with the cyst dyeing technique. (A) Image of a dyed cystic lesion using indigo carmine in the operative field. (B) Image of the operative field after surgical removal of the cyst. (C) Image of the removed cyst with indigo carmine dye.
Case 2
In October 2020, an 80-year-old man complained of severe low back pain and right buttock and leg radiating pain 2 months previously. The pain was given a VAS score of 8. Several block procedures were applied in other hospitals; however, the symptoms prevailed. An L4–5 facet joint synovial cyst compressed thecal sac at the right lateral recess on MRI (Fig. 3).
Preoperative images of a lumbar facet joint synovial cyst at the right L4–5 level on magnetic resonance imaging (MRI). (A) Sagittal image on T2-weighted MRI. (B) Coronal image on T2-weighted MRI.
After informed consent was obtained from the patient, a right unilateral laminotomy for bilateral decompression (ULBD) surgery was performed under general anesthesia. Surgical removal of the cyst using a cyst dyeing method after ULBD was performed successfully. At the upper L3–4 level, ULBD surgery was performed for lumbar spinal stenosis due to lipomatosis. No dural injury was observed. The operative time was about 60 minutes. The patient reported improved low back pain and right buttock and leg radiating pain, which was represented by a reduction in a VAS score from 8 to 1.
Discussion
In these cases, surgical excision with the cyst dyeing technique was successfully performed. The cyst dyeing method was safe and effective, and demonstrated favorable clinical outcomes with no perioperative complications.
Synovial cysts typically develop as a result of degenerative changes that occur with aging. They can be found throughout the spine; however, they are most common in the lumbar region. They are benign, and their histopathology consists of fibrous connective tissue with a synovial cell lining.
Lumbar synovial cysts are observed in 10% of lumbar cases on MRI [7]. However, they are most frequent in the L4–5 facet joint (60%–70%) [8] and less frequent in the intraspinal area (2.3%) [7]. Tarlov cysts, type II meningeal cysts, are more common in the S1 dorsal foramen compared with synovial cysts. Of note, synovial cysts can be differentiated from Tarlov cysts, perineural cysts that form on the nerve root sheath, by continuity from facet joint and their smaller size. Tarlov cysts are characterized by multiplicity, larger size, and lobular contour. Traits of the synovial cyst, including continuity from the facet joint and a singular cyst, were observed in our case (Fig. 1).
Tarlov cysts can occur throughout the spine and are most common in the sacral area of the spine. However, they are generally asymptomatic, and are found incidentally at a frequency of 1% to 2% on sacral MRI [9]. Lumbar facet joint cysts can cause symptoms by compressing the thecal sac and nerve root and causing lumbar spinal stenosis. The symptoms include severe low back pain, radiating pain, and neurogenic intermittent claudication.
There are many treatments for symptomatic facet joint synovial cysts including conservative treatment and surgical excision. The conservative treatments, including resting, taking anti-inflammatory medicine, and applying physical therapy, can often be sufficient. Recently, percutaneous cyst aspiration, steroid injection, and rupture through the facet joint have been implemented in some cases. However, surgical removal for neural decompression is the best procedure for symptomatic lumbar cysts [1–6], although fusion surgery may be needed afterward. By dyeing the cysts with indigo carmine, the anatomical boundary between the cyst and dural sac was clarified (Fig. 2), which allowed their safe separation [10]. Therefore, the cyst dyeing technique is a novel and useful method for symptomatic lumbar cysts.
This study had some limitations. Only 2 cases utilizing the cyst dyeing method were investigated. Therefore, more cases with multi-center involvement, comparison studies, and randomized controlled studies are needed to elucidate the efficiency of the cyst dyeing technique in the future.
Conclusion
The cyst dyeing method is an effective for the surgical removal of symptomatic lumbar spine facet joint synovial cysts.
Notes
Conflicts of interest
No potential conflict of interest relevant to this article was reported.